
Understanding how manual therapy techniques evolve over time deepens our grasp of clinical reasoning and safe application. Lumbar shift correction, also called lateral shift correction or “pig shift” in informal clinical slang (because the position replicates that when carrying a pig on the hip) is a prime example. It’s not just a manoeuvre—it’s a response to a common presentation in acute low back pain and disc-related issues.
Robin McKenzie’s Early Work
The modern roots of lumbar shift correction trace back to Robin McKenzie’s work in the early 1970s. In his 1972 paper on shift correction, McKenzie described a systematic approach to addressing lateral deviations often seen with disc herniations. The technique quickly gained traction in manual therapy circles.
By the late 1970s and early 1980s, the lumbar shift correction appeared in major textbooks. For instance, James Cyriax’s influential Orthopaedic Medicine volumes included lateral deviation and shift correction methods around 1980—sometimes with variations on standing or assisted corrections. These early descriptions emphasised correcting the “list” or scoliosis-like posture to reduce mechanical stress on the disc and nerve roots. Geoffrey Maitland also referenced the lumbar shift correction manoeuvre in his seminal text Vertebral Manipulation.
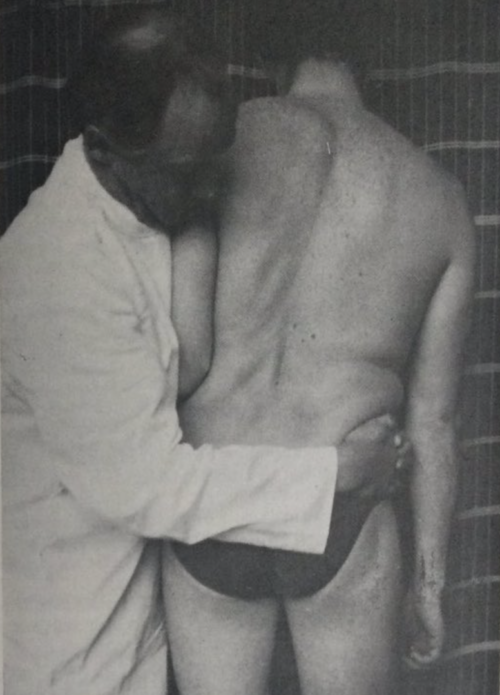
Historical images from those eras (and McKenzie’s original 1972 paper) show the technique has changed little in principle, though delivery has evolved toward patient self-management.
McKenzie’s approach became formalised in his Mechanical Diagnosis and Therapy (MDT) system, with specific “derangement” classifications involving shifts. The author, who taught the McKenzie diploma course for 10 years, respects the foundation but cautions against school-specific dogma.
Shifts are Real and Often Linked to Disc Pathology
Lumbar lateral shifts (visible trunk list or scoliosis secondary to pain) are well-documented and not mythical. They occur in both adults and children. Evidence shows a strong correlation with acute disc herniation or prolapse.
Key studies show:
- Post-surgical lumbar disc herniation cases frequently show persistent shifts that do not self-correct,
- Incidence is significantly higher in adolescents than adults with lumbar disc herniation.
- Shifts can present with or without overt radiculopathy; many occur without clear nerve-root involvement.
Visual detection alone is imperfect; history and movement testing (side-gliding, flexion) are essential. Shifts are not always “antalgic adaptations.” Many patients report more pain or blockage in the shifted position, and gentle correction often provides immediate relief—unlike a learned limp, which persists even when walking backward.
Biomechanics
Shifts correlate strongly with extruded or herniated discs (often on the opposite side of the list). Post-discectomy, some shifts resolve slowly over months even after pain subsides—suggesting a mechanical or protective component beyond simple guarding.
Centralization (symptoms moving toward the spine) and monitoring the most distal symptoms remain critical, especially with radicular pain. The author stresses: “In the presence of radicular pain and radiculopathy the monitoring of the most distal symptoms is always essential, as is knowledge of the centralization phenomenon.”
Correction does not require complex manoeuvres. Patients can often self-correct at home. One variation uses a doorway for upper-trunk stability while side-gliding the lumbar spine—natural spinal motion, no compensation needed.
Correction Techniques
Traditional McKenzie standing shift correction is effective but not the only or always best option. The author rarely uses it in clinic and prefers patient self-correction for home care:
- Side-lying self-correction (“not lying on your pig”) is often gentler and sustainable.
- Hanging or traction variations were historically suggested but are not always indicated (patients may feel temporary relief but worsen on reloading).
- Manual correction followed by maintenance exercises and rehabilitation has case-report support.
Standing shift correction in a door frame is the natural self treatment progression from the lying shift correction procedure. I propose this over the traditional leaning against the wall correction which unloads the patient.
Evidence Base and Updates Over Time
Dozens of studies have shown:
- Natural history of trunk list and McKenzie management influence.
- Radiological characteristics of sciatic scoliosis and recovery after endoscopic discectomy.
- Case reports of alternating shifts, interspinous device complications, and persistent lists post-surgery.
- Narrative reviews on McKenzie mobilization for acute shifts.
- Reliability discussions: Visual assessment alone has limitations; combine with history and active testing.
Conclusion
Lumbar shift correction has evolved from McKenzie’s 1972 descriptions and Cyriax’s textbooks through modern endoscopic surgery studies and patient-centred self-management. Yet the core message remains timeless: listen to the patient, understand the presentation, and prioritise symptom-guided reasoning over any single “school” or manoeuvre.
References
Almeida SD, Menon VV, Vijay SM & Shetty S. (2021). McKenzie mobilisation on acute lumbar lateral shift in patients with low back pain: A narrative review. Journal of Clinical and Diagnostic Research, 15(9), 1-2.
Gillan MGC, et al. (1998). The natural history of trunk list, its associated disability and the influence of McKenzie management. European Spine Journal, 7(6), 480-483.
Kim R, et al. (2015). The incidence and risk factors for lumbar or sciatic scoliosis in lumbar disc herniation and the outcomes after percutaneous endoscopic discectomy. Pain Physician, 18(6), 555-564.
Laslett M. (2009). Manual correction of an acute lumbar lateral shift: Maintenance of correction and rehabilitation: A case report with video. Journal of Manual & Manipulative Therapy, 17(1), 78-85.
Peterson S & Hodges C. (2016). Lumbar lateral shift in a patient with interspinous device implantation: A case report. Journal of Manual & Manipulative Therapy, 24(4), 215-222.
Peterson S & Laslett M. (2021). Alternating lumbar lateral shift. Journal of Manual & Manipulative Therapy, 29(1), 59-66.
Porter RW & Miller CG. (1986). Back pain and trunk list. Spine, 11(6), 596-600.
Sallade J. (1987). Variation on Robin McKenzie’s technique for correction of lateral shift. The Journal of Orthopedic and Sports Physical Therapy, 8(8), 417-420.
Wang L, et al. (2022). Sciatica-related spinal imbalance in lumbar disc herniation patients: Radiological characteristics and recovery following endoscopic discectomy. Journal of Pain Research, 15, 13-22.
Zhu Z, et al. (2011). Scoliotic posture as the initial symptom in adolescents with lumbar disc herniation: its curve pattern and natural history after lumbar discectomy. BMC Musculoskeletal Disorders, 12(216), 1-8.